
TLDR:
-
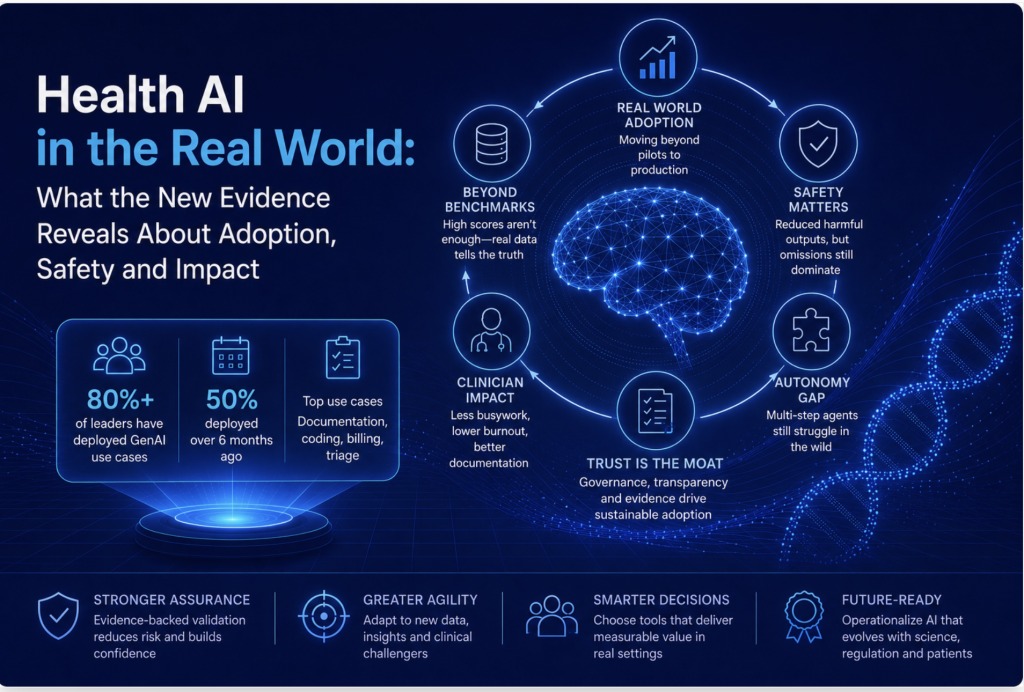
Healthcare AI is no longer experimental: over 80% of leaders have live generative AI use cases, mainly in high‑volume administrative workflows like documentation and coding, so the real challenge is choosing tools that actually work in production.
-
Benchmarks and exam scores are necessary but misleading on their own: most LLM evaluations still rely on synthetic or clean data, and performance drops sharply when models face messy records, real users, and distribution shifts in actual clinical environments.
-
Safety has improved but remains fragile: benchmarks like NOHARM show that even top models can make potentially harmful recommendations in a noticeable fraction of consultations, with most serious errors coming from omissions rather than obvious hallucinations.
-
The clearest ROI today is in busywork, not autonomy: ambient scribes and admin tools already show reduced documentation time, lower burnout, and better reimbursement, while more autonomous, multi‑step clinical agents still struggle to complete end‑to‑end tasks reliably.
-
The real race is trust, not model horsepower: with patients adopting AI faster than institutions can respond, the winning vendors will be those who can prove safety, governance, and real‑world impact, and healthydata.science positions itself as the neutral evidence layer that makes those trust signals visible.
1. Healthcare’s AI moment has arrived
Let’s be honest: finding AI tools for healthcare was never the hard part. There are hundreds of them.
Knowing which ones actually work once they leave the sales deck and walk into a real clinic, that’s the hard part. That’s what our directory exists to solve.
So when ARISE (a research network out of Stanford and Harvard) dropped its first 2026 Healthcare AI Industry Report this July, we read it cover to cover. Not another leaderboard of impressive scores, actual adoption data, safety benchmarks, and real deployment studies. The kind of evidence that tells you what’s happening once these tools leave the lab.
It’s the most useful snapshot of this field we’ve seen. It also confirms a lot of what we already believed about how to vet these tools. Here’s what stood out, and what it means if you’re the one trying to get your organisation to actually use this stuff.
2. Beyond pilots: AI is now part of healthcare operations
2.1 Adoption at scale, not just experiments
Stop asking “should we use AI?” That conversation’s over.
More than 80% of healthcare leaders have already deployed at least one generative AI use case. Half did it over six months ago. This isn’t a pilot cohort anymore, it’s an industry that’s already decided, and moved on to the real question: which tools can we actually trust?
Most of the time, “a use case” isn’t glamorous. A documentation assistant. A coding or billing helper. A triage tool. Nothing flashy, but it’s exactly where the evidence is strongest, because it’s the highest-volume, most repetitive slice of the work.
That’s precisely why curation matters more now, not less. When adoption was rare, picking the wrong tool cost you budget. Now that it’s the default, the risk is patient and clinician safety, at scale.
2.2 The shift from sandbox to production
A pilot and a production deployment get talked about like they’re the same thing. They’re not.
A pilot proves a model can do a task under decent conditions. Production asks harder questions. Does it stay accurate as the patient population shifts? Does it actually plug into the EHR? Is anyone watching it after go-live? Are clinicians using it the way it was designed?
Take TRICORDER, a randomised trial of an AI-enabled stethoscope across 205 NHS practices in the UK. Real promise detecting heart failure, atrial fibrillation, valvular disease. But clinician use was patchy, workflow friction got in the way, and the trial never moved the needle on population-level heart failure detection.
Strong algorithm. Zero real-world impact. That gap is why we push vendors for proof of deployment, not just a slick demo.
3. Benchmarks vs. real-world performance
3.1 Why benchmarks are necessary but incomplete
Benchmarks still matter. They’re the first filter for whether a model even has the medical knowledge worth testing further.
But sit with this: a review of 519 LLM evaluation studies from 2022–2024 found only 5% used real patient data. Fairness, harmful-content risk, administrative accuracy, mostly understudied. A high exam score proves a model can pass a test. It tells you almost nothing about how it behaves in a messy exam room or a chaotic inbox.
Figure 1: Visualising the Reality Gap:
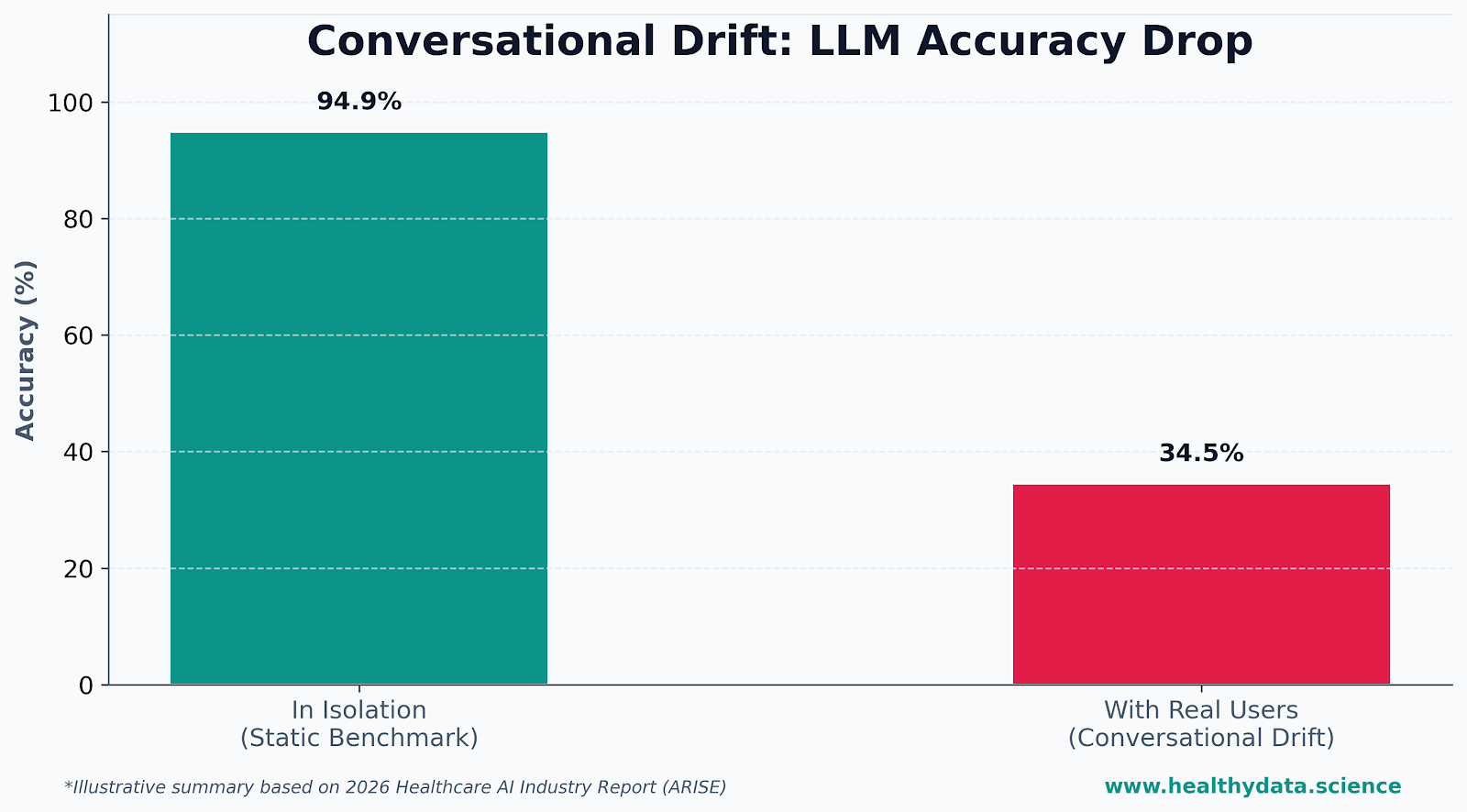
Diagram Summary: As shown in the infographic’s Conversational Drift panel, models that boast a near-perfect 94.9% accuracy rate under clinical test conditions fall flat once they interact with actual patients. In real-world chat environments, accuracy plummets to just 34.5%, proving why static benchmarks alone are a dangerous metric for choosing software.
3.2 The reality of incomplete data and interruptions
Real clinical environments don’t hand a model clean, complete information. Ever. A few examples worth flagging:
→ Conversational drift. Nearly 1,300 people tested LLMs in a randomised study. Accuracy in isolation: 94.9%. Accuracy once real people started actually chatting with the model: below 34.5%. Basically no better than no AI at all (as highlighted above).
→ Multimodal shortcuts. Strip the diagnostic image out of a question that needs it, and several models still scored well above chance anyway. That’s a model leaning on text patterns, not actually “seeing” anything.
→ Distribution shift. A meta-analysis of Epic’s own clinical decision-support tools found real-world performance consistently under what the vendor claimed. Its sepsis model hit an AUROC of 0.65 externally, versus Epic’s reported 0.76–0.83.
None of this is hallucination in the classic sense. These are failures that only show up once a tool meets messy records, distracted users, or a population it was never built for.
3.3 How our directory evaluates beyond benchmarks
For us, a benchmark table is where a listing starts, not where it ends. We want deployment metrics from live settings. Independent evaluations, not just vendor-funded ones. Documented error analysis. Evidence of a rollback or override switch if things go sideways after launch.
| Benchmark-only vendor | Real-world evidence vendor | |
|---|---|---|
| Evidence type | Static test sets, synthetic cases | Prospective deployment data, live workflow studies |
| Population tested | Often unspecified or narrow | Matched to actual patient mix |
| Failure reporting | Rarely disclosed | Structured incident and error analysis |
| Post-launch monitoring | Not addressed | Defined cadence, drift detection |
4. Safety: improving, but still fragile
4.1 What the NOHARM results actually mean
The report leans hard on NOHARM. A benchmark built to measure clinically harmful AI outputs, tested head-to-head against real physicians instead of in isolation.
Across 100 real consultation cases, even the best models produced recommendations with the potential for severe harm in roughly 1 in 14 consultations. For the weakest models, that jumped to nearly 1 in 4. But here’s the context that matters: the top models still beat generalist physicians evaluated on the same cases. So the question isn’t “is AI perfect.” It’s “is AI safer than the alternative a patient would otherwise get.”
4.2 Missing information as the dominant failure mode
Here’s the finding that deserves way more airtime: over 80% of NOHARM’s serious errors came from failing to recommend something necessary. Not from making stuff up. A separate 2026 Stanford evaluation of an agentic discharge-summary tool found the same thing. Hallucinations, just 2%. Omissions, a full quarter of cases.
Omission is just harder to catch than hallucination. There’s no glaring wrong answer to flag. A model that forgets to ask about pregnancy status, or misses declining kidney function before recommending a drug, doesn’t look wrong on the surface. It just looks… fine. Until it isn’t.
So before we vet any clinical decision support tool, we want proof it actively prompts for missing info, flags its own uncertainty, or escalates when it’s out of its depth.
Figure 2: Visualising the Safety Threat
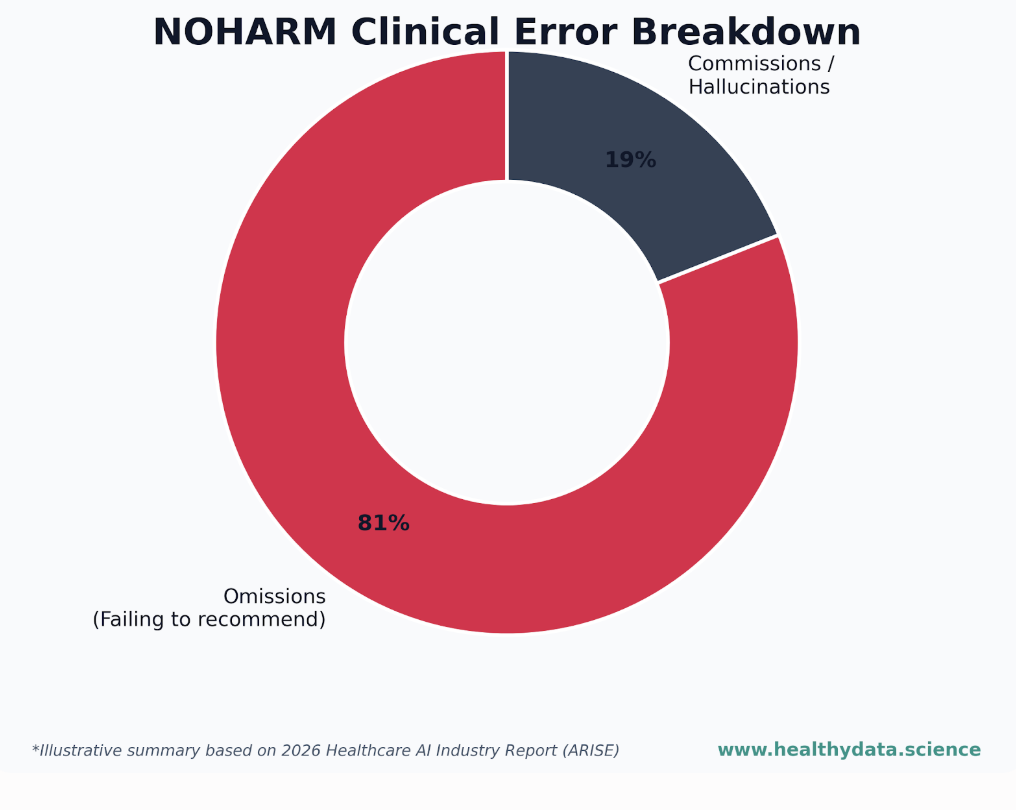
Diagram Summary: While the industry frequently worries about “hallucinations,” the ARISE data highlighted in the NOHARM Serious Errors panel tells a different story. An overwhelming 81% of severe clinical AI errors are silent omissions, failing to ask for or recommend crucial clinical information. While only 19% stem from active hallucinations or incorrect commissions.
4.3 Safety signals our directory requires from vendors
“We’re built on a frontier model” isn’t a safety claim. It’s a starting point. Before we mark a listing safety-vetted, we need to see:
→ Structured harm analysis or incident reporting. Not just marketing copy about accuracy → Clear human-in-the-loop and escalation paths, built per task, not applied as a blanket rule → Explicit limits on autonomy in higher-risk workflows → Governance and auditability — can a decision be traced and reviewed after the fact
A big model with no safety engineering behind it? That’s an unvetted model, full stop.
5. Where AI adds the most value today: busywork, not autonomous decision-making
5.1 The administrative sweet spot
The clearest wins in this whole report are administrative. No contest.
Across five academic medical centres, ambient scribe adoption meant less documentation time, a small bump in visit capacity, and a consistent drop in reported physician burnout. That’s the gap between a scribe that reliably writes a good note and a system trying to diagnose patients on its own. One’s proven at scale today; the other’s still earning its evidence.
Here’s a stat worth bringing to your steering committee: this isn’t just about saving time. Ambient scribes can actually increase per-visit reimbursement by capturing clinical detail that used to go undocumented. One health system saw an 11% jump in physician work relative value units after rollout. Real upside, but also a good reason to ask vendors how their tool affects coding, not just hours saved.
5.2 Autonomy is coming, but the bar is higher
More autonomous workflows, triage, treatment recommendations, multi-step agentic tasks, are improving fast. The evidence just isn’t there yet.
On HealthAdminBench, a benchmark for agentic admin tasks, the best-performing agent finished only 36.3% of end-to-end tasks successfully with portal guidance, and 19.3% without it. That’s the same system that scored 82.8% on individual subtasks tested in isolation. Nailing one step doesn’t mean nailing the whole chain.
Which is exactly why we classify listings by autonomy level: assistive, semi-autonomous, autonomous, instead of throwing everything under one “AI-powered” label.
Figure 3: Visualising the Autonomy Drop-off
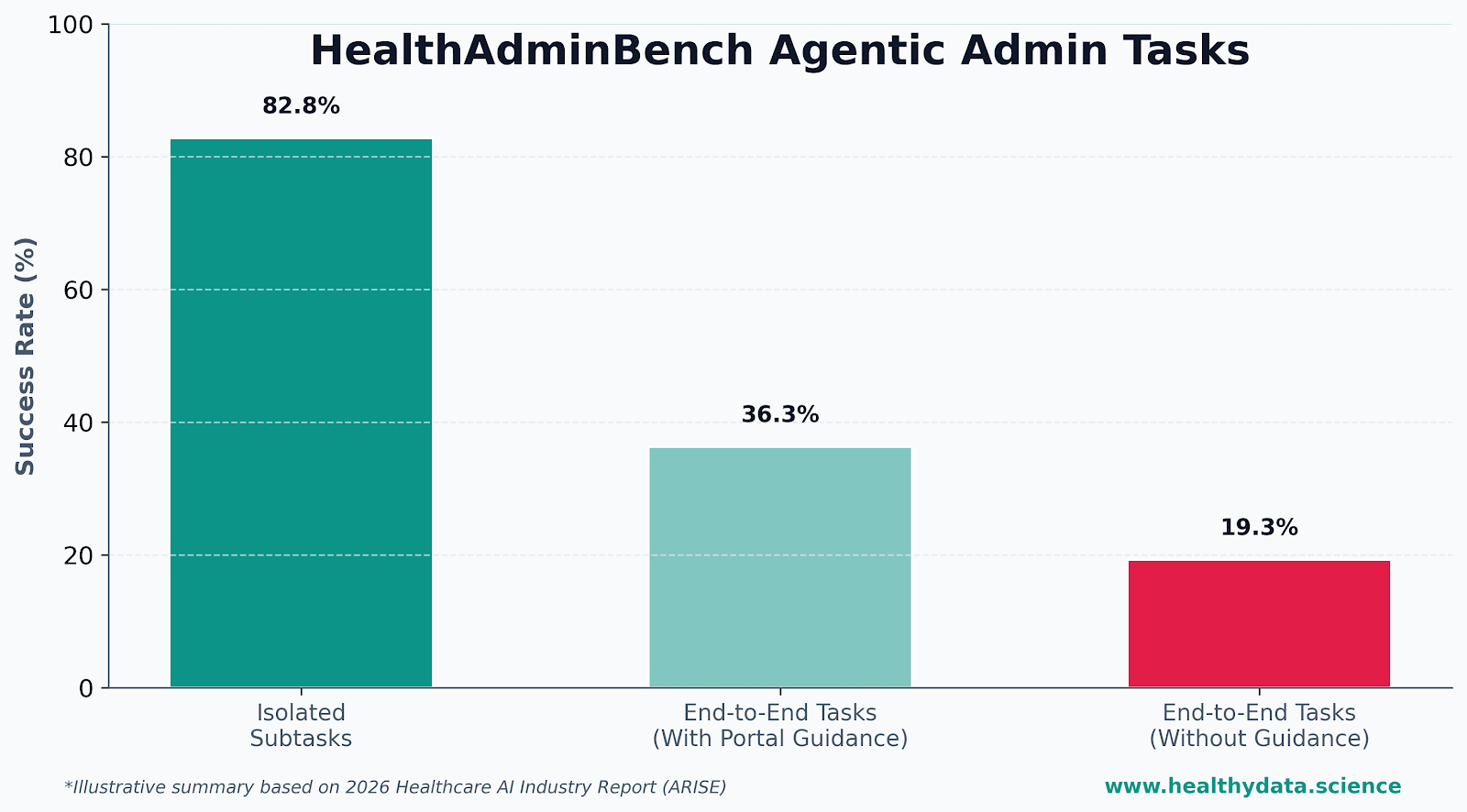
Diagram Summary: The Agentic Admin Tasks panel illustrates why multi-step clinical workflows are not ready for full autonomy. While an AI agent can successfully execute isolated subtasks 82.8% of the time, its success rate drops to 36.3% when guided through an end-to-end portal workflow, and collapses to just 19.3% when running entirely unassisted.
5.3 Matching use cases to evidence
We filter by task category (documentation, coding, triage, research, patient messaging, more), autonomy level, and strength of clinical validation. Why? Because most of the buyer frustration we hear about comes down to a mismatch, a tool proven safe for low-risk documentation gets pushed into a high-risk decision-support role it was never tested for.
Not every listing needs that lens, though. A validation or eQMS platform, for example, isn’t making clinical decisions, so we don’t force it into a clinical-autonomy framework it doesn’t belong in. What stays consistent across every listing type is the underlying discipline: real deployment evidence, documented risks and limitations, and a straight comparison against the alternatives, just built around the questions that actually matter for that category of tool.
6. Patients are moving faster than the system
6.1 Consumer adoption: AI as a routine health advisor
Public use of AI chatbots for health has roughly doubled in a year. About a third of US adults now turn to AI chatbots with physical or mental health questions, skewing younger. Some of the biggest adoption jumps came from groups the health system has historically struggled to reach.
The pattern’s pretty consistent: symptom checking, interpreting lab results, medication questions.
6.2 The growing gap between expectations and institutional response
Trust hasn’t caught up with usage, and that’s the real story here. Only about half of people trust AI chatbots. Nearly half say they’re uncomfortable with providers using AI in their care. And yet patients increasingly show up to appointments with AI-generated explanations already in hand. A lot of them never follow up with an actual clinician at all.
High use. Low trust. Uneven follow-through. Put those together, and you get friction, contradictory guidance, unmanaged misinformation, and more work for clinicians answering AI-shaped questions they didn’t even prompt.
6.3 Vendor responsibilities in patient-facing contexts
For patient-facing tools, we ask the obvious questions. Is this built for real comprehension? Plain language, adapted for literacy and language barriers? Is there a clear line between what patients see and what clinicians see? Does the vendor actually track how patients interpret and act on what the tool tells them?
Worth remembering: global chatbot adoption is still a minority activity. Only around 16% of the world’s population had used a generative AI tool by late 2025. Accessibility and health literacy design aren’t a bonus feature, they’re table stakes for the access this whole industry keeps promising.
7. The real race: proving trust, not just improving models
7.1 Why “better models” is no longer enough
Models keep getting smarter. The report cites frontier models meeting or beating physician-level performance on a growing set of benchmark tasks. But here’s the catch: capability and deployment readiness have quietly split apart.
The report’s own MAST evaluation found that stronger overall model capability doesn’t reliably predict safe clinical behaviour. Doing well on static reasoning tests doesn’t mean doing well on multi-step agentic tasks inside a real EHR. Going forward, the winning vendor isn’t the one with the newest model. It’s the one who can prove, with actual evidence, that their tool is safe in a real care setting.
Even the labs building these tools seem to agree. Cameron Chen and Mike Schaekermann, who lead Google’s AMIE team, put it plainly: they believe in studying medical AI through a phased, safety-first approach. AMIE didn’t jump straight from benchmark to bedside. It moved through simulated conversations, OSCE-style testing, and a small monitored patient cohort before expanding into larger real-world trials. If a team building frontier medical AI treats staged evidence as non-negotiable, that’s a pretty strong signal for how the rest of us should be evaluating, and rolling out these tools too.
7.2 What trustworthy vendors show you
A short list worth running past every healthcare AI vendor you talk to:
→ Can you show results beyond your own benchmark — ideally something independently verified? → What are this tool’s defined operating boundaries, and what happens when it hits them? → Do you monitor performance after deployment, and how often do you review it? → How does your evidence map to recognised frameworks, like WHO’s AI ethics principles or your own institution’s governance process?
7.3 How our directory operationalises trust signals
We turn vendor documentation into structured, comparable profiles: an evidence section separating vendor-reported benchmarks from actual deployment case studies, a documented risks-and-limitations section, and, where it’s relevant to the tool. Safety and governance fields like human-in-the-loop design, escalation paths, and autonomy alignment.
For clinical decision-support tools, that means clinical validation and autonomy tier.
For compliance and validation platforms, it means things like audit-trail depth, regulatory alignment, and data governance controls instead. The framework flexes to the category, but the underlying bar (show us real evidence, not just claims) doesn’t.
We’re not trying to predict who has the “best” model. Nobody can reliably do that six months out anyway. We’re trying to help you see who can actually prove their tool works safely where it’ll actually be used.
8. Conclusion
Healthcare AI is past the pilot phase. Adoption’s real. Capability’s real. Investment’s real. What hasn’t caught up is the proof that any of it works safely at scale. And even the report’s own conclusion says the bottleneck now is evidence and trust, not algorithms (which our directory is built upon).
The organisations that win with AI in 2026 won’t be the ones chasing the newest model. They’ll be the ones who asked the harder questions before they deployed anything.
Vendors: send us your evidence, benchmarks, clinical studies, deployment data, safety artefacts. And get evaluated alongside your peers.
Buyers: use the directory as a neutral evidence layer next time you’re weighing tools for documentation, coding, triage, research, or patient-facing work.
This article draws on the ARISE 2026 Healthcare AI Industry Report (July 2026, Stanford/Harvard). Full report and citations at arise-ai.org.

Author: Stephen
Founder of HealthyData.Science · 20+ years in life sciences compliance & software validation · MSc in Data Science & Artificial Intelligence.