

TLDR
AI‑governed robotic fill‑finish uses digital‑twin models and simulations to design and optimise robot motion and airflow inside Grade A aseptic cells, rather than only applying AI to downstream visual inspection.
The concept aims to shift contamination control and human‑intervention reduction upstream into system design and control logic, potentially supporting safer, more flexible small‑batch biologics and ATMP fill‑finish once validated.
Current evidence is engineering‑focused (motion planning, dynamic CFD, trajectory optimisation) and remains at proof‑of‑concept stage, with no GMP outcome data yet on deviations, media fills, or yield.
Evaluation should focus on integration complexity across motion‑planning, CFD and optimisation tools, robustness of digital‑twin assumptions, and how the AI/simulation stack can be validated under Annex 1 and GMP expectations.
Key risks include regulatory acceptance, concentration of advanced capability in large pharma/CDMOs, workforce reskilling demands, and the need for clear cross‑functional governance of AI‑influenced Grade A decisions.
This article explores an emerging, next‑generation clinical AI concept that is not yet available for purchase or routine commercial use.
AI‑governed robotic fill‑finish is shifting from futurist vision to early engineering reality [1]. Aseptic fill‑finish has always been a “small error, huge impact” step in the life‑sciences value chain: one particle, a slight airflow disturbance, or a mis‑stoppered vial can undo years of upstream work and put patients at risk [4]. Emerging work on digital‑twin‑guided, AI‑optimised robotic aseptic cells points to a new wave of innovation where robots don’t just repeat fixed motions under human supervision; they’re designed, tested, and continuously optimised in silico, with airflow, first‑air protection, and contamination risks modelled before a single batch is run [1, 5].
This draft looks at one such concept: Helbling’s digital‑twin‑guided robotic aseptic cell [1]. It’s not a commercial product, but it does offer a concrete, technically credible glimpse of what “AI‑governed fill‑finish” could mean in practice [6]. The aim isn’t to sell a specific platform; it’s to unpack the clinical and operational problem, the emerging AI approach, the early evidence, and the risks and roadblocks on the path from simulation to routine GMP use, exactly the kind of deep‑dive you’d expect to find on HealthyData.science.
Why sterile fill‑finish is ripe for AI and robotics
Aseptic fill‑finish is one of the most tightly controlled and heavily scrutinised stages in injectable manufacturing [11]. By the time the product reaches this step, it’s survived years of R&D and complex upstream processing; it’s then exposed, transferred into final containers, and sealed [4]. Any lapse in aseptic technique or equipment performance can mean batch rejection, product shortages, or direct patient harm [2].
Two trends are pushing current practice to its limits.
First, the shift from large, predictable batches to smaller, more diverse runs, biologics, high‑potency drugs, and advanced therapy medicinal products (ATMPs). Makes every unit more valuable and every intervention more critical [10].
Second, regulators and industry alike recognise that human interventions in Grade A/B environments remain a major contamination risk, even with isolators and strict gowning; yet operators are still needed to handle exceptions, unusual formats, and late‑stage changes that rigid automation can’t manage well [3].
Against this backdrop, AI‑enabled robotics is a compelling proposition [8]. Robots could take on more of the delicate, repetitive, or hazardous tasks in Grade A spaces, guided by models that anticipate airflow disturbances, optimise motion, and cut down avoidable human interventions [1]. The real question for a sceptical manager or steering committee isn’t “Is AI cool?”, it’s:
“How do we get from today’s fixed recipes and inspection‑only AI to systems where intelligent software helps design and, eventually, govern what robots do inside the isolator?” [9].
Inside an AI‑optimised robotic aseptic cell
Helbling’s article, “A Quality by Design approach optimises automation in aseptic production,” is one of the clearest public examples of how digital twins and AI‑style optimisation can be applied to robotic aseptic cells [1]. Rather than starting from a finished machine and bolting on monitoring tools, the team builds a virtual model of the cell, robot arms, isolator geometry, airflow, and critical zones. And uses that as a testbed for design and optimisation decisions [5, 6].
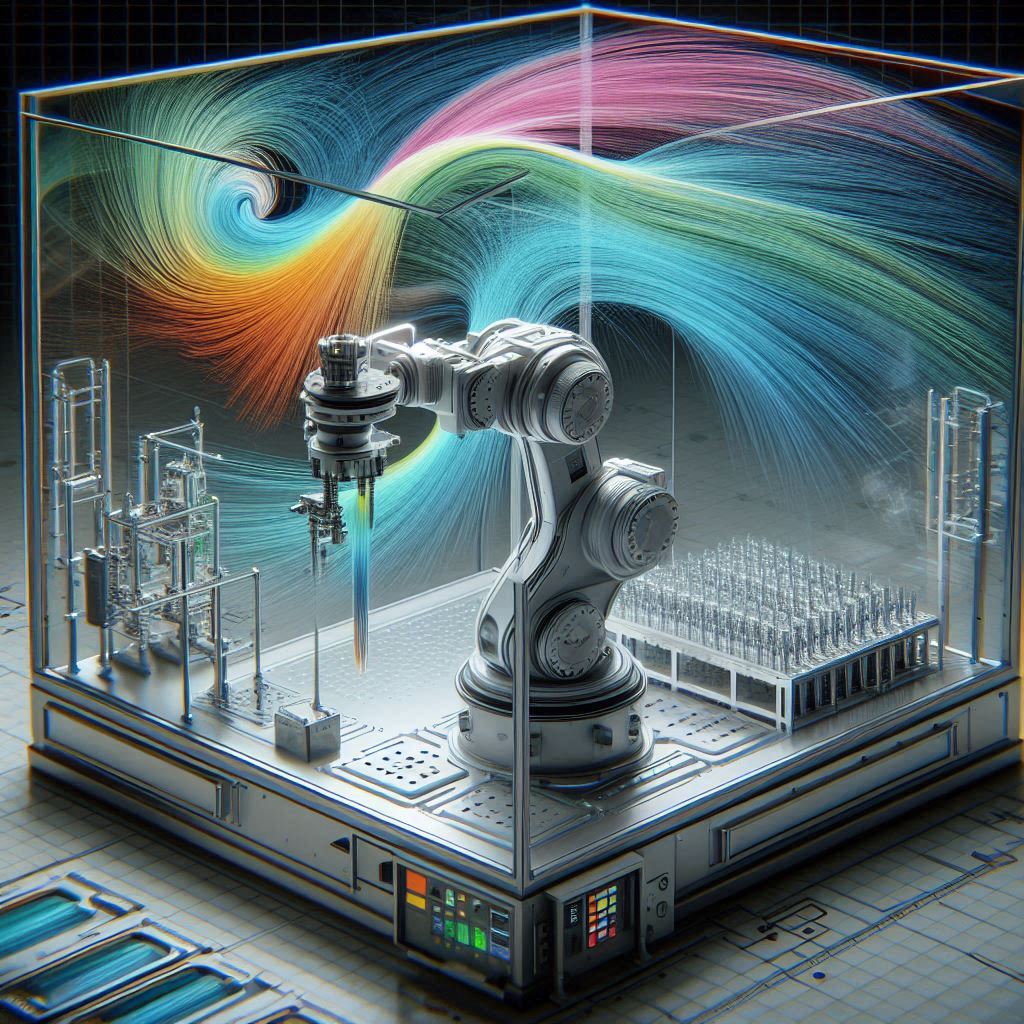
At the heart of the approach is a dynamic digital twin. Robot trajectories are planned with motion‑planning tools, then passed into computational fluid dynamics (CFD) simulations that model how moving arms and grippers disturb laminar airflow and first‑air protection [1]. By simulating different paths, speeds, and tool designs, engineers can see where vortices and turbulence might appear long before any physical hardware is built or validated [1].
One key insight from the Helbling case study is simple but powerful: motion matters. Static airflow models may suggest that an isolator layout is compliant, but only dynamic CFD with moving components reveals how real robot motions can momentarily disrupt Grade A conditions [1]. As the authors note, “Dynamic CFD can capture phenomena such as vortices and turbulence, which may not be revealed if motion is not accounted for” [1]. That’s exactly the kind of insight that invites AI‑assisted optimisation: algorithms can be tasked with finding trajectories that hit process goals while minimising risky airflow patterns [1, 9].
In this prototype, the AI element is less about black‑box decision‑making and more about intelligent optimisation, with the digital twin acting as the environment where candidate solutions are iteratively evaluated and improved [13]. In principle, this optimisation loop could evolve into a ‘sense–simulate–decide–act’ control cycle, where sensor data from the real cell updates the twin, and the twin informs incremental adjustments to robot behaviour [7, 13].
How this differs from today’s AI‑enabled fill‑finish

It’s important to separate this emerging approach from how AI is used in filling lines today. Right now, AI is most visible in automated visual inspection (AVI) and related quality control tasks [12]. Deep learning models are trained to spot particles, cosmetic defects, or fill‑level anomalies in vials and ampoules, complementing or replacing rigid rule‑based image processing [12]. Vendors showcase impressive gains in detection accuracy and fewer false rejects, but this AI still sits at the edge of the process, flagging defective units after they’re filled [9].
Other Pharma 4.0 initiatives add AI assisted cameras, vibration sensors, and IoT connectivity to monitor equipment health and process conditions [7]. These systems feed dashboards, alarms, and maintenance schedules, helping operators run lines more efficiently and reduce unplanned downtime [2]. In some forward-looking scenarios, a vision system might detect a misaligned stopper and automatically trigger a robotic correction upstream, hinting at closed‑loop control [3].
By contrast, the digital‑twin‑guided robotic cell concept embeds intelligence into the design and control of the aseptic environment itself [1]. Instead of just watching for problems, an AI-optimised system tries to prevent them by shaping how the robot moves and interacts with airflow from the start [1, 8]. That makes it a different category of AI involvement. Closer to AI as part of the “governor” of the process than AI as an aftermarket monitor [13].
For readers used to clinical AI tools that interpret images or predict risk scores, this might feel like a subtle but important shift. Here, AI’s job is to co‑design a physical system and its control policies under strict GMP constraints, not just spit out a classification [14]. It opens up new possibilities, but also brings fresh validation and governance questions that HealthyData.Science can help unpack.
What the evidence shows so far

Here’s the reality check. Right now, evidence for AI‑governed robotic fill‑finish is much more engineering-driven than clinical or regulatory. Helbling’s publication is essentially a detailed case study: it walks through motion planning, mesh generation, boundary‑condition setup, dynamic CFD simulation with moving components, and trajectory optimisation [1]. The outcome is a convincing demonstration that this integrated approach can spot airflow risks and support compliant designs for robotic interventions in Grade A / ISO 5 settings [1, 6].
What it doesn’t yet provide are the dataset‑style metrics GMP and clinical audiences are used to. There are no charts showing reduced media fill failures, fewer deviations, or better right‑first‑time fills vs conventional setups [1]. There’s also no multi‑site pilot data or post‑implementation reviews from live commercial production. That’s understandable at this stage, but it means claims about patient or business impact are still largely extrapolated [2, 10].
In the broader literature, digital twins and simulation are widely promoted as enablers of advanced manufacturing, and AI‑based inspection systems report strong accuracy on specific tasks like fill‑level or defect detection [12, 14]. Very few public sources, however, describe in Helbling‑level detail how motion, airflow, and robot design are co‑optimised via simulations and intelligent tooling [1].
For now, the most honest characterisation is that this is a promising proof‑of‑concept that strengthens the engineering toolkit for aseptic automation, not a proven clinical‑impact story. The next frontier will be well‑designed pilots where AI‑optimised trajectories are used in media fills and real product runs, with outcomes measured against meaningful quality and reliability metrics, a potential topic you can explore further in longer articles on HealthyData.Science.
Risks and roadblocks on the way to routine use
Letting AI influence or govern what happens inside a Grade A isolator is obviously not risk‑free. On the technical side, integrating motion‑planning tools, CFD solvers, and optimisation algorithms with robotic controllers creates complex dependency chains [1]. Each interface, data formats, time steps, control signals, can become a point of failure or brittleness if it’s not carefully engineered and validated [1]. As Helbling notes, “integrating different software tools into this process involves combining heterogeneous, non-trivial interfaces” and needs an iterative procedure [1].
From a sterility perspective, the digital twin is only as good as its assumptions about airflow, boundary conditions, and robot behaviour [1, 4]. If the model underestimates turbulence in certain modes or misses real‑world obstructions and wear‑and‑tear, it might falsely reassure engineers that conditions are safe. In short, a poor twin could hard‑code a false sense of security.
Regulation adds another layer. Annex 1 and core GMP principles demand that manufacturers understand and control all critical parameters affecting sterility [11]. That’s uncomfortable territory for opaque or constantly learning models [14]. Even if the optimisation is deterministic and well documented, regulators will expect solid rationales for how trajectories are chosen, how changes are managed, and how the twin is kept aligned with reality over time [7]. Validation teams will need methods to verify not just the robot and isolator, but also the simulation and optimisation stack.
There are system‑level and ethical questions, too. Highly complex AI‑robotic cells may only be viable for large pharma and CDMOs, widening gaps in manufacturing capability between regions [2, 13]. If only a small group of manufacturers can deploy the safest, most flexible fill‑finish setups, access to some high‑value therapies could become even more uneven. At the same time, the workforce will need to move into new roles around data, automation, and validation, with responsibilities and accountability clearly defined [15].
A glimpse of the future: expert perspectives
Despite the challenges, many industry voices see AI‑driven robotics as an inevitable part of future aseptic manufacturing [8, 9]. Innovation‑focused suppliers talk about a shift from robots simply replacing human hands to robots operating in interconnected, data‑rich networks of sensors and AI systems [3]. In that kind of environment, AI doesn’t work in isolation; it taps into IoT data, advanced analytics, and real‑time monitoring to maintain quality targets [7].
Conceptual frameworks like Pharma 4.0 argue that IoT, advanced analytics, and automation should collectively support higher drug‑product quality, with real‑time data enabling smarter control [7]. One summary notes that IoT “empowers and augments these factors in a unified fashion where data is tabulated, accessible, and comprehensive, and monitoring and feedback can occur in real time” [7]. That’s exactly the type of ecosystem where AI‑optimised digital twins could thrive.
Practitioners are also candid about the human side. Commenting on robotic production in Zurich, one observer asked,
It’s a throwaway line that neatly captures a quality of life argument, freeing people from demanding environments, and the broader shift toward machines taking on more of the physical burden under strict controls [15].
What needs to happen next
To move AI‑governed robotic fill‑finish from engineering papers into routine practice, a few things have to come together. First, pilots that go beyond “it works in simulation.” These should combine AI‑optimised robotic trajectories with standard aseptic validation exercises, media fills, environmental monitoring, and intervention logging, to quantify outcome differences vs conventional setups [3, 10].
Metrics could include contamination events, deviation rates, unplanned interventions, and overall yield across different product types.
Second, robust validation frameworks for digital twins and AI components [1]. That means treating the twin as a regulated model with documented assumptions, verification tests, and change‑control procedures, and ensuring any optimisation logic is transparent enough to audit [7]. Manufacturers will need playbooks for updating models when line layouts change, new formats are introduced, or unexpected behaviours appear.
Third, alignment with evolving AI and advanced manufacturing guidance [14]. Regulatory sandboxes, position papers, and joint industry–regulator initiatives can clarify expectations and acceptable validation strategies, reducing uncertainty for early adopters [13]. Lessons from clinical AI governance, on transparency, robustness, and human oversight, could accelerate fit‑for‑purpose frameworks on the manufacturing side.
Finally, cross‑functional engagement is crucial. QA/QP, clinicians focused on product availability and safety, digital and data teams, and manufacturing engineers all have a stake in how AI‑governed systems are introduced. Agreeing on success criteria and risk tolerances up front will make it easier to have grown‑up conversations with vendors.
For teams monitoring developments in AI in healthcare and life sciences, HealthyData.Science provides independent explainers of emerging AI solutions in healthcare and approaches. Content is informed by practical project experience and research, helping teams build informed awareness and assess developments internally.
References
- Helbling. A Quality by Design approach optimizes automation in aseptic production. January 2025.
- CDMO World. Optimizing Fill–Finish Operations in Modern Biopharmaceutical Manufacturing. January 2025.
- BioPharm International. Automating the Future of Fill/Finish. March 2024.
- Chemtech. The 1‑2‑3 Guide to Aseptic Fill Finish Manufacturing. June 2024.
- Helbling. Pharma & Biotechnology – Automation and Digitalization in Regulated Industries. January 2025.
- Aargau Economic Development. Helbling supports innovation in pharmaceutical production. January 2025.
- AST. Implementing Pharma 4.0 Solutions for Fill-Finish. February 2025.
- West Pharmaceutical Services. AI‑Driven Robotics in Pharma Manufacturing for Improved Safety. January 2026.
- Optima. AI innovations in pharmaceutical production. February 2025.
- GenEngNews. Automation and AI Help Meet Demand for Biologics Fill-Finish Services. August 2023.
- BioPharm International. Prepping Fill/Finish Systems to Ensure Quality Output. October 2020.
- Intuition Labs. Computer Vision in Pharmaceutical Quality Control: Enhancing Drug Manufacturing. April 2024.
- McKinsey. Reimagining life science enterprises with agentic AI. January 2025.
- PMC. Artificial Intelligence (AI) Applications in Drug Discovery and Drug Development. October 2024.
- LinkedIn – Nicolò Borromeo. Pharma manufacturing and the rise of robots. January 2025.

Author: Stephen
Founder of HealthyData.Science · 20+ years in life sciences compliance & software validation · MSc in Data Science & Artificial Intelligence.